

Here’s the number that matters before we get to any drug: there are three transactions hiding under the word “peptides,” and only one of them has a name attached to it when something goes wrong. I spent time sorting through the 2026 rulebook the way I sort through any dataset, by finding the variable that actually predicts the outcome. That variable is not price, and it’s not how clinical the website looks. It’s whether a licensed clinician’s name is on the file.
This piece links every regulatory and clinical claim to a primary source. It is not legal advice, and it is not written by a clinician. Last reviewed June 2026.
The one question that sorts the whole market
Ask this before anything else: is a licensed clinician writing you a prescription, or isn’t there one in the picture at all?
That single binary splits the entire peptide market into two populations with wildly different risk profiles. Prescription drugs are legal to obtain when a licensed clinician evaluates you and prescribes, and a licensed pharmacy fills the order. Doesn’t matter if it’s an FDA-approved finished product or a compounded preparation, the mechanism is the same. Pull the clinician out of the transaction and you’re not buying medicine anymore. You’re buying a chemical, and you’ve walked into a different rulebook entirely.
So my checklist starts with a search, not a read: find the prescriber on the page. If they’re there, you’re in a supervised lane. If the checkout flow never mentions one and the label says “research use only” or “not for human consumption,” you’re in the unsupervised lane, and everything downstream changes.
Lane 1: FDA-approved, and the trial numbers to prove it
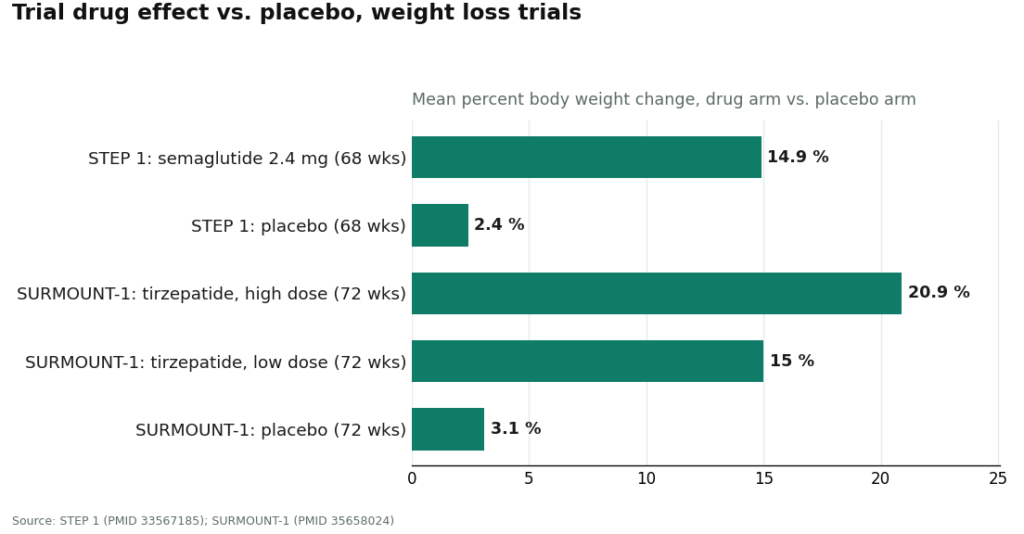
Semaglutide and tirzepatide are the cleanest data points in this whole category, so let’s start there. In the STEP 1 trial, adults on semaglutide 2.4 mg weekly lost a mean 14.9% of body weight at 68 weeks, against 2.4% on placebo [1]. That’s a net drug effect of about 12.5 percentage points once you subtract the placebo response, a number the source data lets you compute even though nobody states it outright.
SURMOUNT-1 pushes that further. Tirzepatide produced mean reductions of 15.0% to 20.9% across its dose range over 72 weeks, against 3.1% on placebo [2]. Do the same subtraction at the top end and you get roughly 17.8 points of net effect at the highest dose, the largest gap in the comparison.
| Trial | Drug arm (mean loss) | Placebo arm | Net effect | Duration |
|---|---|---|---|---|
| STEP 1 [1] | 14.9% (semaglutide 2.4 mg) | 2.4% | ~12.5 pts | 68 weeks |
| SURMOUNT-1 [2] | 15.0%–20.9% (tirzepatide, by dose) | 3.1% | ~11.9–17.8 pts | 72 weeks |
This lane is legally the easiest to reason about. Clinician, prescription, pharmacy, done. The tradeoff isn’t legal risk, it’s price. Branded approved product sits at the top of the cost curve in this category, which is precisely the pressure that pushes people toward the next two lanes.
Lane 2: compounded, on a prescription
Most informed buyers end up here, and it’s the lane most often misread. Compounding is a licensed pharmacy preparing a medication tailored to a specific patient. It’s a real, regulated category, not a loophole. When a licensed clinician prescribes a compounded peptide and a licensed pharmacy fills it, the transaction sits inside a recognized legal structure.
But there’s a variable you have to hold constant in your head: compounded drugs are not FDA-approved, and the FDA has not evaluated them for safety, effectiveness, or quality before they reach you [3]. That’s not a legality problem. It’s a different risk profile than an approved drug, operating under a different set of rules that the law explicitly permits through licensed pharmacies.
What that means in practice, reduced to two facts: a compounded peptide obtained through a real prescription and a licensed pharmacy is a legal transaction. And the protection you’re actually buying is licensure and oversight, not an FDA stamp on that specific vial. A provider who states both of those facts up front is giving you a complete picture. One that markets its compounded product as functionally identical to the approved version is skipping the exact distinction the 2026 enforcement wave cared most about.
FormBlends operates in this lane: a licensed clinician reviews you, decides whether to prescribe, and a licensed compounding pharmacy dispenses if appropriate. I’m naming it here as an example of what the compliant structure looks like from the buyer’s side, not as a recommendation. Nothing here is for sale, and there’s no checkout to click through.
Lane 3: the research-chemical market
Now the lane where the legal confusion actually concentrates. A meaningful share of peptide sales online happen under a “research use only” or “not for human consumption” label. That label isn’t decorative. It is the entire legal position of the seller, stated in writing.
Run the logic through: by selling the vial as “research,” the seller sits outside the framework that governs medicines. No prescription, no clinician, no licensed pharmacy, no one checking that the vial contains what it claims. When you buy it and use it on yourself, you’ve stepped outside the lane the seller carefully stayed inside of. The risk transfers to you completely, and it stays there.
Here’s the part I’d flag as a data person: the lower price in this lane is not a discount on an equivalent product. It’s the price of a product with every protective layer stripped out, no evaluation, no accountable party if the contents are wrong. Read the disclaimer as a warning label, because that’s functionally what it is.
A simple scoring table for any offer you see
Rather than a paragraph of caveats, here’s how I’d score any peptide page in under a minute, across four checks:
| Check | Legal lane (pass) | Chemical lane (fail) |
|---|---|---|
| Prescriber named on page? | Yes, evaluates you first | No mention |
| Label language | “Prescription” or “compounded by licensed pharmacy” | “Research use only” / “not for human consumption” |
| States compounded ≠ FDA-approved [3]? | States it plainly, unprompted | Silent, or implies equivalence |
| Named, licensed dispensing pharmacy? | Yes | No, unnamed supplier + seller certificate |
Four yeses puts you in a legal, supervised lane. Any no is a data point worth weighting heavily, regardless of how polished the surrounding site looks.
What actually moved in 2026
If the market feels tighter, that’s because enforcement, not the underlying law, sharpened. Through early 2026, regulators focused on marketing that blurred compounded and approved products together, or that obscured who was actually compounding and dispensing. The compounded lane itself didn’t become illegal. What changed is the signal-to-noise ratio: a compliant operator in 2026 is now more likely to state outright that compounded products aren’t FDA-approved, name its licensed pharmacy, and keep a real clinician in the loop. An operator still using equivalency language or hiding the prescriber is showing you exactly the pattern regulators were watching for.
The pick, stated plainly
If I’m ranking the three lanes by legal clarity and risk transfer: FDA-approved on prescription is the cleanest data point, unambiguous but the most expensive. Compounded on a real prescription through a licensed clinician and licensed pharmacy is legal and materially cheaper, with the clearly stated caveat that the FDA hasn’t evaluated that specific preparation [3]. Research-chemical purchases sit outside both frameworks, and the full risk is yours the moment you use the product on yourself.
Run the four-point check before you spend anything. Find the clinician, read the label, demand the FDA-approval disclosure, locate the pharmacy. That’s the whole test, and it’s the only one that actually predicts which lane you’re standing in.
The questions I get most
Is peptide therapy legal in the United States? Yes, when a licensed clinician prescribes it and a licensed pharmacy dispenses it. FDA-approved peptides on prescription are straightforwardly legal, and compounded peptides through a licensed clinician and pharmacy are legal too, with the stated caveat that compounded products aren’t FDA-approved and haven’t been evaluated for safety, effectiveness, or quality [3]. Buy a “research use only” vial and use it yourself, and you’ve moved outside that framework. The risk is entirely yours.
Are compounded peptides legal even though they’re not FDA-approved? Yes. Compounded peptides prescribed by a licensed clinician and prepared by a licensed pharmacy are legal under the conditions the law allows. “Not FDA-approved” doesn’t mean illegal, it means the agency hasn’t evaluated that specific preparation for safety, effectiveness, or quality before it reaches you [3]. Your protection is the licensure and oversight, not an FDA stamp on the vial.
What does “research use only” actually mean on a peptide label? It’s the seller telling a regulator, in writing, that the product was never meant for a human. No prescription, no clinician, no licensed pharmacy in the chain. Once you use it on yourself, the responsibility for that crossing is entirely yours. Treat the label as a warning, not paperwork.
Is it illegal to buy peptides without a prescription? The seller stays on the legal side of the line by labeling the product “for research use only,” which moves the transaction outside the medicine framework. The exposure shifts to you the moment you buy and use the vial, since there’s no clinician, no licensed pharmacy, and no accountable party if the contents are mislabeled or contaminated. The lower price reflects stripped-out protections, not a discount on the same product.
How do I score a peptide seller for legality in under a minute? Run the four-check table: named prescriber who evaluates you first, label language (“compounded by licensed pharmacy” versus “research use only”), a plain statement that compounded meds aren’t FDA-approved [3], and a named, licensed dispensing pharmacy. Four passes puts the offer in a legal lane.
Did the law on compounded GLP-1 peptides change in 2026? The compounded lane itself wasn’t outlawed. Regulators through early 2026 tightened focus on marketing that blurred compounded and FDA-approved products together, or hid who actually compounded and dispensed them. Practically, that means a trustworthy operator in 2026 states plainly that compounded products aren’t FDA-approved, names its licensed pharmacy, and keeps a real clinician involved.
Primary sources
- Wilding JPH, et al. “Once-Weekly Semaglutide in Adults with Overweight or Obesity” (STEP 1). New England Journal of Medicine, 2021. PMID 33567185. Mean weight loss 14.9% on semaglutide 2.4 mg vs 2.4% placebo at 68 weeks. https://pubmed.ncbi.nlm.nih.gov/33567185/
- Jastreboff AM, et al. “Tirzepatide Once Weekly for the Treatment of Obesity” (SURMOUNT-1). New England Journal of Medicine, 2022. PMID 35658024. Mean weight reduction 15.0% to 20.9% across doses vs 3.1% placebo over 72 weeks. https://pubmed.ncbi.nlm.nih.gov/35658024/
- U.S. Food and Drug Administration. Human Drug Compounding guidance. Compounded drugs are not FDA-approved and have not been evaluated by the FDA for safety, effectiveness, or quality.
How much does peptide therapy typically cost?
By my read of the publicly reported ranges, peptide therapy generally runs $150 to $600 or more per month, depending on the specific peptide, the dose, and the source. Physician-supervised programs cluster at the higher end of that band, because the price is covering clinical oversight and lab work, not just the compound itself. Regional variation and how many peptides are bundled into a protocol both move the number too.
Does insurance cover peptide therapy?
Almost never. Most peptides used in wellness and anti-aging protocols aren’t FDA-approved for those indications, so insurers file them as elective or experimental and decline to pay. A narrow exception exists for specific peptides, like certain growth hormone formulations prescribed for a diagnosed deficiency, where partial coverage sometimes applies. That’s the exception, not the pattern. Budget for out-of-pocket.
How much does BPC-157 therapy cost, and is it even legally available right now?
The price data here has shifted because the FDA placed BPC-157 on a list of bulk drug substances compounding pharmacies can’t use without specific authorization, a restriction that tightened heading into 2026. Back when it was more widely compounded, monthly cost ran roughly $80 to $250. The legal supply chain right now is genuinely unsettled, which means a low quoted price through an unregulated seller deserves real scrutiny, not less.
Is peptide therapy actually worth the cost?
That depends on what you’re comparing it against, and how honestly you weigh the evidence for the specific peptide in question. Some have solid clinical backing for defined conditions, others are used well ahead of the research supporting them. A supervised protocol with baseline labs, clear goals, and a clinician adjusting the plan based on your results has real accountability built into the price. Buying unvetted powder online doesn’t carry that same math. A conversation with a physician who specializes in this area, such as those working through a compounding pharmacy like FormBlends, is the fastest way to get a realistic read on your specific case.
Written by Junia Yang, reporting fellow. Last reviewed April 2026.
General educational content. Speak with a licensed professional before changing your routine.



